|
Applied Kinesiology Muscle Testing
How to determine in advance which medicine |
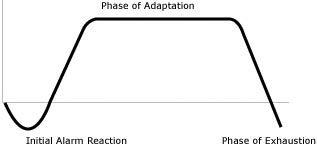
Abstract: German (and Austrian) medical doctors discover how to use Applied Kinesiology muscle testing to produce reliable, repeatable, statistically well-correlated medical analysis. They recommend that the results of such muscle testing should not be used alone for diagnosis, but rather as a useful complement to standard lab tests. Doctors know that the medicine which works best for one patient may prove to be ineffective for another patient with the same presenting symptoms and diagnosed syndrome. Knowing this phenomena, doctors often tell their patients some variation of, "Take this prescription for two weeks. If your condition doesn’t improve, come back and I’ll write a prescription for another medicine that may help." Is there any way to know in advance which medicine will be most effective? A group of chiropractors and medical doctors in the United States, the International College of Applied Kinesiology (ICAK), claim that they can use manual muscle testing to test which medicines will be effective for specific patients. Attracted by this promise, a group of medical doctors in Germany and Austria subjected Applied Kinesiology techniques to the most critical analysis. This research was spearheaded by Wolfgang Gerz, a medical doctor in Munich, Germany. They determined that many popular kinesiology techniques as well as many of the techniques that the ICAK promotes as valid did not stand up to double-blind testing. Through further experimentation, they have developed techniques that produce significantly accurate results. These techniques are very useful for medical diagnosis and the results can be reproduced by any doctor who takes the time to learn them. These German doctors experimented with the gentle type of muscle testing promoted by the popular lay kinesiology groups such as "Touch for Health". Most of the people using this kind of muscle testing are laypersons who therefore speak of themselves as "testers", not therapists or doctors. And for the same reason they have "clients" not patients. In this kind of muscle testing, the tester initiates the muscle test and applies a gradually increasing force upon the limb of the client for about two seconds. It is then the client’s job to stabilise his limb and provide increasing counter-pressure at exactly the same rate as the tester so the tested limb does not move during the test. Thus in order to perform this kind of muscle testing, the client must be initially trained to react with neither too much nor too little force. And the client must be trained to neither apply his force too slowly nor too swiftly. The burden of responsibility is thus upon the client, who is often new to muscle testing. Since (hopefully) the tester is more experienced than the client, placing so much responsibility upon the client increases the probability of error. Although some testers seemed to be able to utilise this kind of muscle testing with good results, the correlation of results between testers was not significant enough for trustworthy medical analysis. When the doctors experimented with this kind of testing, they found that when each of them muscle-tested the same individual independently, they did not significantly agree as to which muscles tested strong and which tested weak. Therefore, they abandoned this popular type of muscle testing. The doctors also experimented with the standard medical muscle test described by Kendall and Kendall. While in medical school, most doctors learned to diagnose with this kind of muscle testing. For example, after an injury to the spine, a doctor will test the muscles that are innervated by the segment of the spine that was injured. If these muscles cannot adequately contract and thus test weak, this result is considered to be evidence that the injury may have caused a pinching or other damage to the nerves supplying these muscles. This medical muscle testing was further developed by Dr. George Goodheart, the founder of the ICAK. For simplicity, this kind of muscle testing will be called here "AK muscle testing". In AK muscle testing, the patient initiates the contraction of the muscle and presses as hard as he can. The patient doesn’t suddenly push but rather increases the force he applies up to a complete contraction over a period of 1-2 seconds. It is the doctor’s responsibility to provide adequate counter-pressure (isometric resistance) so that the limb remains in the beginning position. When the doctor senses that a complete contraction has been achieved, the doctor then applies a small amount of isotonic pressure against the fully contracted muscle. If the patient can react by contracting his muscle a bit more than his normal maximal contraction, the muscle tested strong. If the patient cannot meet this extra demand, the typical reaction is that his muscle contraction will suddenly break and limb will move. In this case, his muscle is said to have tested weak. The German doctors did a double-blind study using AK muscle testing. They each independently tested various patients and compared their results. The doctors were able to achieve a very significant 90% correlation of results. Thus AK muscle testing was chosen for further inquiry. Most Touch for Health-type muscle testers and most therapists using AK muscle testing simply assess if a muscle tests either strong or weak. Strong is considered to be good and weak to be inadequate or bad. However, in medical analysis, all factors have a sub-normal range, a range in which they are considered normal, and above that a range in which they are considered excess. Whether it is the rate of the heartbeat, the blood pressure, the sugar level in the blood or any other bodily factor, there is always a level above which the rate or amount of the factor tested is considered excess (too high or too much). Therefore, if muscle testing was to be made useful for medical diagnosis, a way to detect the excess states, to determine if a muscle tests "too strong", needed to be developed. Hans Selye, in his classic studies of stress, noted that the typical reaction to stress is an initial drop in energy. Selye calls this the alarm phase. Then, if the stress continues, the body produces extra cortisols (adrenaline etc) which increases the tone; the tension in the skeletal muscles. Selye calls this the phase of adaptation. If the stress is chronic, there comes a time when the body is exhausted and cannot produce the elevated levels of cortisols. Selye calls this the phase of exhaustion. Selye’s state of adaptation involves muscles that are in a state of excess tension. This provided a hint toward determining the muscles that test "too strong". |
 |
|
The Three Stages of Reaction to Stress - Hans Selye
|
Until recently, the literature of AK had only scanty references to muscles testing too strong and no defined way to test for this state. In fact, there was no agreed upon definition of what muscle testing is. Gerz tackled these problem head on. With his group of doctors plus David Leaf (ICAK), a working definition of AK muscle testing was written in 1994 (Gerz, p. 11). |

Muscle Testing Rectus Femoris |
|
|
| Also in 1994, in the meeting of the ICAK-D leaders in Monte Carlo, hypertonic muscles and methods for detecting hypertonic muscles were defined (Gerz, p. 15). Follow this link for illustrations of these methods. These definitions are presented in a simplified manner below: Hypertonic, in AK, has a slightly different meaning than in medicine. In medicine, a hypertonic muscle is one in which the state of tonus is too high. Such a muscle feels tight and hard to palpation and often is painful, either to palpation, to movement or all of the time. A hypertonic muscle in AK refers to a muscle that tests strong but cannot be made to test weak by one of four means: 1) Stimulation (touching during the muscle test or tapping immediately prior to the muscle test) of the sedation point for the meridian associated with the specific muscle. 2) Approximation (pinching) of the spindle cells in the belly of the muscle, parallel to the contractile fibers which usually lie parallel to the long axis of the muscle. 3) Stroking the associated meridian in the opposite direction to its natural flow, from its end towards its beginning. 4) Placing one or the other pole of a 3000 gauss magnet upon the belly of the muscle. Stimulation of the sedation point was determined to be the most trustworthy method of detecting hypertonic muscles, with pinching of the spindle cells coming in a close second. Only when a muscle tests strong, but can be weakened by one or more of the above four methods, is it considered a candidate for use as an indicator muscle, a "normotonic" muscle, for other diagnostic purposes. So, the results of Applied Kinesiology muscle testing are: Weak - Muscle tests weak - Inadequate contraction Normotonic - Tests strong, can be weakened - Optimal contraction Hypertonic - Tests strong, cannot be weakened - Excess contraction Now the doctors had, with this type of muscle testing, an instrument for determining the three states common to all medical diagnosis. They then applied this to various diagnostic inquiries and developed useful protocols. Note the similarity between these three results and the three stages of stress defined by Hans Selye. The next challenge was to determine if AK muscle testing could be used in a trustworthy way to test allergens, nutrients, medicines and other remedies. Popular kinesiologists muscle test the effect of substances by having their clients hold them in the hand. The doctors open-mindly tested this method. Surprisingly, they obtained significantly similar results when testing most children and some adults in this way. When testing most adults with hand-held substances, the results were not well correlated. However, when a tiny quantity of the substance to be tested was placed upon the tongue of the subject, the results were not only nearly identical between the doctors, they also corresponded well with standard lab tests. In one study, known allergens which when injected under the skin formed a characteristic allergic bump were presented, double-blind, orally, and the results were assessed with muscle testing. Oral presentation of the allergens caused a normotonic indicator muscle to weaken. There was a very significant 80% correlation between the known allergens and those detected by muscle testing. Allergic substances were not always detected by muscle testing. This indicates that medical diagnosis by muscle testing alone is not adequate and will miss some important results. Interestingly, some substances that produced no skin reaction, did weaken indicator muscles. This result implies that substances can have a negative effect upon bodily function without causing allergic reactions. Since neither method found all problems, the use of both standard lab tests and muscle testing is recommended. How are these new techniques applied in a daily medical practice? Let’s say that blood tests have revealed that a patient has a significant deficiency of zinc. Since zinc is required by the stomach, thymus, pancreas and the reproductive organs, the doctor will first test muscles known to be related to these organs. These muscle-organ/gland correspondences were first discovered in the mid-1960s by George Goodheart. He found, through observation of his patients, a statistical correlation between specific organic dysfunctions and imbalances in the function of specific muscles. These correlations have been verified by extensive research. Later he was surprised to find that his correlations were identical to the correlations between the organs and the meridians, expounded thousands of years earlier in Chinese medicine. Here are ones relevant to our example: Stomach: Pectoralis major clavicularis Thymus: Infraspinatus Pancreas: Latissimus dorsi Reproductive organs: Piriformis, Gluteus maximus, Gluteus medius, Adductors |
 |
 |
 |
 |
|
Pectoralis major clavicularis
|
Infraspinatus
|
Latissimus dorsi
|
Piriformis |
| If one or more of the above muscles tests either weak or hypertonic, it may be used as a possible indicator for the zinc deficiency. Various chemical combinations of the nutrient zinc in the form of zinc citrate, zinc ascorbate, zinc picolinate, zinc orotate etc., are place one at a time upon the tongue and the previously imbalanced muscle is again tested. If the tested substance produces any change of the muscle test results, the mouth is rinsed with water and the muscle is again tested. When the effect of the tested substance is now eliminated and the muscle again tests weak or hypertonic as it did at the beginning of the session, further testing can proceed. The particular form of zinc that makes the muscle test normotonic is considered to be the preferred one for supplementation by that patient at that time. Methods for testing the proper dosage do not yet exist in AK. The recommended dosage is prescribed through the doctor’s knowledge of orthomolecular medicine plus considerations such as body size and other individual factors related to his patient. Other related nutritional factors that may be needed (such as copper with zinc or vitamin D and calcium with magnesium) are tested together with the determined form of the deficient nutrient in the patient’s mouth at the same time. As long as these extra nutrients do not cause the muscle to weaken or test hypertonic, they are also prescribed "en bloc". Experience has shown that the particular nutrients and the specific chemical combinations of them that the body requires and "chooses" through AK muscle testing may change in a matter of days. For this reason, the testing and prescribing procedure is repeated after a duration of one to two weeks. In cases of pain, the proper nutrient or medicine upon the tongue will often not only make a related muscle normotonic, but will often immediately reduce the pain. If more than one substance makes the related muscle normotonic, the one that most reduces the pain is prescribed. Case history: A female patient had shoulder pain which was exacerbated during the muscle testing of teres minor. Teres minor is related to the thyroid gland which requires iodine for proper function. |
 |
|
Testing Teres Minor
|
| Oral potassium iodide had no effect upon muscle strength. A natural source of iodine, the sea weed fucus vesiculosus, placed upon her tongue not only made teres minor normotonic, but also immediately reduced the pain and increased the range of motion. Various other sources of iodine were tested, one at a time. The sea weed formula, Algasan®, produced the greatest reduction of pain and the greatest increase in range of motion and was therefore prescribed. This aspect of AK muscle testing increases patient compliance. When the patient experiences an immediate improvement of symptoms with the tested remedy in her mouth, the probability that she will take it as recommended increases significantly. The AK protocol for the diagnosis and treatment of an overgrowth of the yeast, candida albicans; a common medical problem today. Since the overgrowth of candida occurs primarily in the small intestine, the rectus femoris, a functionally strong and easily tested muscle associated with the small intestine meridian and organ is a logical choice. If the rectus femoris tests strong but cannot be weakened by sedation point tapping (= is hypertonic), this indicates that the organ associated with the rectus femoris, the small intestine, is likely stressed and in a state of adaptation (Selye). Stress to the small intestine is often caused by dysbiose, an imbalance of the flora that live there. The most common culprit is Candida albicans. We all have candida albicans living in our intestines. However, an overgrowth can cause a plethora of the common symptoms plaguing people today including headaches, joint pains, exhaustion, depression etc. A hypertonic testing rectus femoris is evidence to suspect a possible overgrowth of candida. |
|
|
 |
|
Testing the Rectus Femoris
|
Tapping the Sedation Point for Rectus Femoris
|
| To determine if candida is the causative factor, a tiny bit of the antigen of candida is placed upon the tongue of the patient. Then the hypertonic rectus femoris is again tested. If it now "breaks" and tests weak, this is considered strong evidence that the small intestine is currently stressed by an overgrowth of candida. The results of this test are statistically well-related to the results of lab culture tests of fecal matter and dark-field blood tests for candida. Actually, stool tests are notorious for often not detecting existing candida overgrowths. Judging by the health improvement through proper consequent treatment, even when candida was not found in the stool test, the AK test for candida may be more accurate than the stool test. As long as the candida antigen remains in the mouth, the rectus femoris will continue to test weak. This is an ideal condition to test for a remedy for the candida overgrowth. The doctor will typically test the weakest, most natural anti-yeast substances first and move to more potent ones until the least toxic effective remedy is determined. The substance which, when also upon the tongue, causes the rectus femoris to test normotonic (strong but can be weakened), will be effective as an anti-candida treatment for this patient and is a candidate for prescription. Anti-fungal remedies or medicines that do not make the rectus femoris normotonic will not be as effective for the particular patient. Those that have no strengthening effect at all will likely be ineffective. Those that make the weakened rectus femoris hypertonic may have undesirable side effects. Note that the same substance will not necessarily make the weakened-by-candida-antigen rectus femoris test normotonic in another patient with the same symptoms. What we have here is a method to determine which remedy will work best for a particular patient. Extensive protocols for using this method for many medical syndromes and diseases have been developed and used with success. In general, a weak-testing muscle related to the disturbance must be located and used. The relationship between specific muscles and organs provides one approach. Otherwise, the doctor may have the patient touch, press upon or otherwise "challenge" the bodily area where the medical problem is located and simultaneously test most any normotonic muscle for weakening. If the indicator muscle now tests weak, the challenge is continued while possible remedies are placed, one at a time, upon the tongue. Rinsing the mouth between tests may be necessary. The remedy that makes the indicator muscle normotonic is the one to prescribe. These are but a few examples of how medical doctors are using Applied Kinesiology muscle testing in their medical practice. Using these procedures, theoretically logical but ineffective prescription is avoided. The prescriptions are individually tested which means that patients receive their individually most-effective form of nutrients, remedies or medicines in the first prescription. The observed results of application of this protocol in terms of speed of healing are encouraging. Evidence indicates that through using these methods, the doctor can determine, in advance, precisely which nutrients, remedies or medicines will work best for his patients. The ICAK-D offers complete training courses (about 150 hours) for licensed therapists of all kinds. For more information, contact ICAK-D, Leopoldstr. 33, D-80802 München, Tel 068 381 00310, Fax 089 38100318, http://www.ICAK-D.de. It’s affiliate, the IMAK, offers a 160 hour training program in Applied Kinesiology for medical doctors and dentists. Contact IMAK, St. Veiter Str. 34, A-9020 Klangefurt Fax 0043 463-514242 or IMAK Buro Deutschland, Sonnenlängstr. 2, D-81369 München, Tel: 089 780 9824, Fax 089 781 928. Are interested in learning Applied Kinesiology but you cannot, at this time, take the time away from your busy medical practice for such training? If so, you can get a good introduction to Applied Kinesiology and its techniques in the reference and training book, Grundlagen der Applied Kinesiology, by Robert Frost (ISBN 3-932098-27-7). The English version, Applied Kinesiology: A Training Manual and Reference Book of Basic Principles and Practices (ISBN 1-55643-374-4) is now published by North Atlantic Press, Berkeley, California. For a description of the English version of the book and ordering information, click here. For further information contact him by email: . Further information about Applied Kinesiology is available on his website: http://joyousworld.com/health/ak |
| References: Frost, Robert: Grundlagen der Applied Kinesiology, VAK-Kirchzarten, Germany, 1998. Frost, Robert: Applied Kinesiology: A Training Manual and Reference Book of Basic Principles and Practice, Berkeley, CA, North Atlantic Press, 2002. |